 Prostate cancer is the commonest non-skin cancer in men in the UK. It is different from most cancers in that a significant proportion of men, particularly older men with a shorter life expectancy, have a non-aggressive form of this cancer, meaning that it is unlikely to cause symptoms or progress beyond the prostate gland during their lifetime. Sometimes in younger men the cancer can be small, slow growing and present only a limited risk to the patient. Clinically important prostate cancers can be defined as those that threaten the well-being or life span of a man.
Prostate cancer is the commonest non-skin cancer in men in the UK. It is different from most cancers in that a significant proportion of men, particularly older men with a shorter life expectancy, have a non-aggressive form of this cancer, meaning that it is unlikely to cause symptoms or progress beyond the prostate gland during their lifetime. Sometimes in younger men the cancer can be small, slow growing and present only a limited risk to the patient. Clinically important prostate cancers can be defined as those that threaten the well-being or life span of a man.
Often prostate cancer does not produce any symptoms, or it may produce symptoms similar to benign enlargement of the prostate, BPH. These include:
Most patients are diagnosed with prostate cancer after they are found to have a raised PSA (prostate specific antigen) blood test, or because they have an abnormal feeling prostate. However,the PSA test is not entirely accurate. There is no real safe lower limit. Even in men with “normal” levels of PSA (less than 3 to 4 ng/ml) around 15% may have small prostate cancers. Conversely, the PSA level may be increased by conditions other than the presence prostate cancer, such as BPH or prostatitis (infection in the prostate).
A multi-parametric MR imaging test (mp-MRI) has been shown to identify areas in the prostate suspicious for cancer. Mp-MRI uses 2-3 sophisticated interpretations of digital information from the scan to allow the radiologist to identify these abnormality. It is now known that the accuracy of MRI is superior to any laboratory test available so far. Although the quality is outstanding, mp-MRI cannot diagnose prostate cancer alone and it also cannot fully exclude prostate cancer either. A biopsy is most commonly still required. However, it can give valuable information regarding the risk of prostate cancer, if it is normal, and suspicious areas can be targeted using MRI-US fusion technology. CUP works closely with the Radiologists at Addenbrooke’s Hospital who are accredited experts in reading Prostate mp-MRI.
Men should undergo an mp-MRI first. This will allow an initial assessment prior to transperineal prostate biopsy using guidance by fusion the MRI to the life ultrasound. Few patients will need to undergo a TRUSP prostate biopsy in order to establish the diagnosis of prostate cancer. Prostate biopsy involves taking several cores of prostate tissue using an ultrasound probe placed in the rectum, and is usually done under a short general anaesthetic.The biopsy will give information such as the grade of the tumour (how aggressive the cancer looks), which is called the Gleason score.
A microscopic picture of a prostate biopsy showing a Gleason grade 3 tumour. The grade is determined by what the cells look like under the microscope.
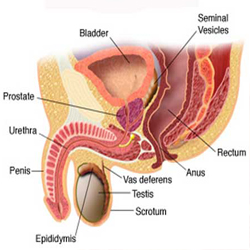
After a diagnosis of prostate cancer further tests may then need to be done to determine the stage of the disease. This tells your doctor whether the disease has spread. Such tests might include an MRI scan, CT scan and/or bone scan and PSMA PET scan. Once the grade and stage have been established, you will be able to discuss with your urologist which treatments are suitable.
Staging tests will help determine if the cancer has spread outside the prostate, and if so how far.
There may be a number of suitable treatments, and for patients with suitable localised disease these might include:
For advanced or metastatic disease, the options may include:
Brachytherapy involves implanting tiny pellets which release low level radiation into the prostate in an attempt to kill of cancer cells whilst sparing healthy surrounding tissue. This technique also offers itself to be used as focal therapy.
MRI Fusion transperineal prostate biopsies & Brachytherapy
To: Mr Kastner and Dr Russell
I am very privileged to have met you and benefitted from your extensive knowledge and very high level of expertise in urology and prostate cancer.
My experience of your consultations, assessment and subsequent treatment was exceptional.
I left with the impression that the service I received was personalized and of the highest standard and have the confidence that I have received the best treatment from the best doctors in the world.
I was particularly impressed with the sense of urgency from top down, including Andrew Styling, your secretaries and of course the staff in the Addenbrooke’s Treatment Centre.
Thank you
Kind regards
At Cambridge Urology Partnership we are able to offer suitable men who choose radical prostatectomy as their preferred treatment option a robotically assisted laparoscopic prostatectomy, also known as robotic surgery for prostate cancer. This has the advantages over traditional open prostatectomy of shorter hospital stay, less pain, less risk of infection, less blood loss and transfusions, less scarring, faster recovery and quicker return to normal activities. For more information on this please read our guide to treatment options for men with localised prostate cancer and see our information sheet about robotically assisted laparoscopic prostatectomy, or robotic surgery for prostate cancer.
Oncologists
Urologists:
Mr DR aged 63
"11 months after my "radical prostatectomy" robotic assisted op performed by Mr Shah, and the three months of aftercare with Mr Shah and Sr Basnett, I would like to express my gratitude for their professionalism and genuine concern. It is always a pleasure to return to see them! Thanks to them I now feel that I can look forward to a healthy life ahead! They deserve the highest praise for the valuable work they do. Thankyou so much!"
Mr PG
"Dear Mr Shah, I would like to thanks you and your team for the care and attention I received from the outset of the robotic prostatectomy including my hospital stay and aftercare. Following the operation I was surprised how quickly I was up and about, with very little discomfort internally and the small external wounds only taking a couple of weeks to heal. I was able to return to work just four weeks after the operation, (most helpful as I am self-employed). But I think that the best thing other than the removal of the cancer is the speed with which my waterworks have recovered. Once again I would like to thank you for taking my case, and for a very satisfactory outcome of the operation."
For patients who have not had a diagnosis of prostate cancer made:
Below are two nomograms that help determine the risk of prostate cancer in patients who have not had a diagnosis of prostate cancer made :
Recently a risk calculator has become available for men with suspected PCa based on an abnormal DRE or elevated PSA. It predicts the probability of a positive biopsy, including the probability of a high grade (high Gleason score) biopsy. It takes into account
This risk calculator is based on the Prostate Cancer Prevention Trial (PCPT). In this study, 5519 older men with a relatively low PSA ( = 3 ng/mL) who did not receive active treatment for 7 years had a 6-core biopsy.
This risk calculator currently consists of 2 prostate risk indicators accessible to patients. They predict the probability of a positive biopsy. They take into account
Risk indicator 1
Risk indicator 2
The Prostate Risk Indicator is based on data from 6288 Dutch men aged 55-74 years living in Rotterdam and participating in the European Randomized Study of Screening for Prostate Cancer (ERSPC) [2]. These men were tested for serum PSA and for any prostate abnormalities by DRE and TRUS and were subsequently followed-up over time.
For patients who have a diagnosis of prostate cancer:
The best known nomograms to help predict pathological stage are below. The risk calculators are developed for men who have had a positive biopsy but have not yet received active treatment (e.g. radical prostatectomy, radiation therapy or hormone therapy). They are trying to answer the questions:
To use these risk calculators, the following clinical data should be available:
Note that these tables are based on a population of patients from the USA , and as such may not translate to patients from elsewhere.
This is best-known risk calculator for predicting pathological stage. This risk calculator takes into account
It is based on data from 5000 patients who underwent radical prostatectomy by a single surgeon at Johns Hopkins in the US .
2. Center for Prostate Disease Research Tables (CPDR)
Similar to the Partins Tables, the CPDR Tables predict pathological stage based on pre-operative clinical parameters:
In contrast to Partins tables, they are based on a more racial diverse US population who underwent surgery at multiple institutions.
3. Memorial Sloan-Kettering Cancer Center (MSKCC) or Kattan pre-treatment nomogram
The Kattan pre-treatment nomogram helps to predict pre-operatively pathological stage based on
Further information about prostate cancer can be found at the following sites
Macmillan cancer backup information on prostate cancer
Cancer Research UK: prostate cancer
Holmium for BPH : about the holmium laser
Lumenis website: information about HoLEP (holmium laser enucleation of the prostate)
The Da Vinci Robot for radical prostatectomy, or robotic surgery for prostate cancer
The Prostate Cancer Network: a patient-led Support Group whose aims are to improve the diagnosis, treatment, care and support to those affected by prostate cancer.
The Prostate Cancer Charity: the UK’s leading voluntary organisation working with people affected by prostate cancer. There are a number of excellent information sheets provided by them, and direct links to these can be found at the bottom of this page.
Prostate UK: fund medical research, the training of healthcare professionals and provide information on all prostate diseases
NICE guidance on prostate cancer
The Prostate Cancer Foundation: funds research into prostate cancer and has information about prostate cancer.
Orchid: Orchid exists to save men's lives from testicular, prostate and penile cancers through pioneering research and promoting awareness
UK Prostate Link: a resource site for prostate cancer information